The idea
Cardiovascular diseases (CVD) are the leading causes of death globally. Risk factors for CVD are routinely measured in population surveys. This provides an opportunity to study health transitions. Understanding the drivers of health transitions can generate knowledge on where resources may best be directed to reduce the burden of disease.


Aims & Objectives
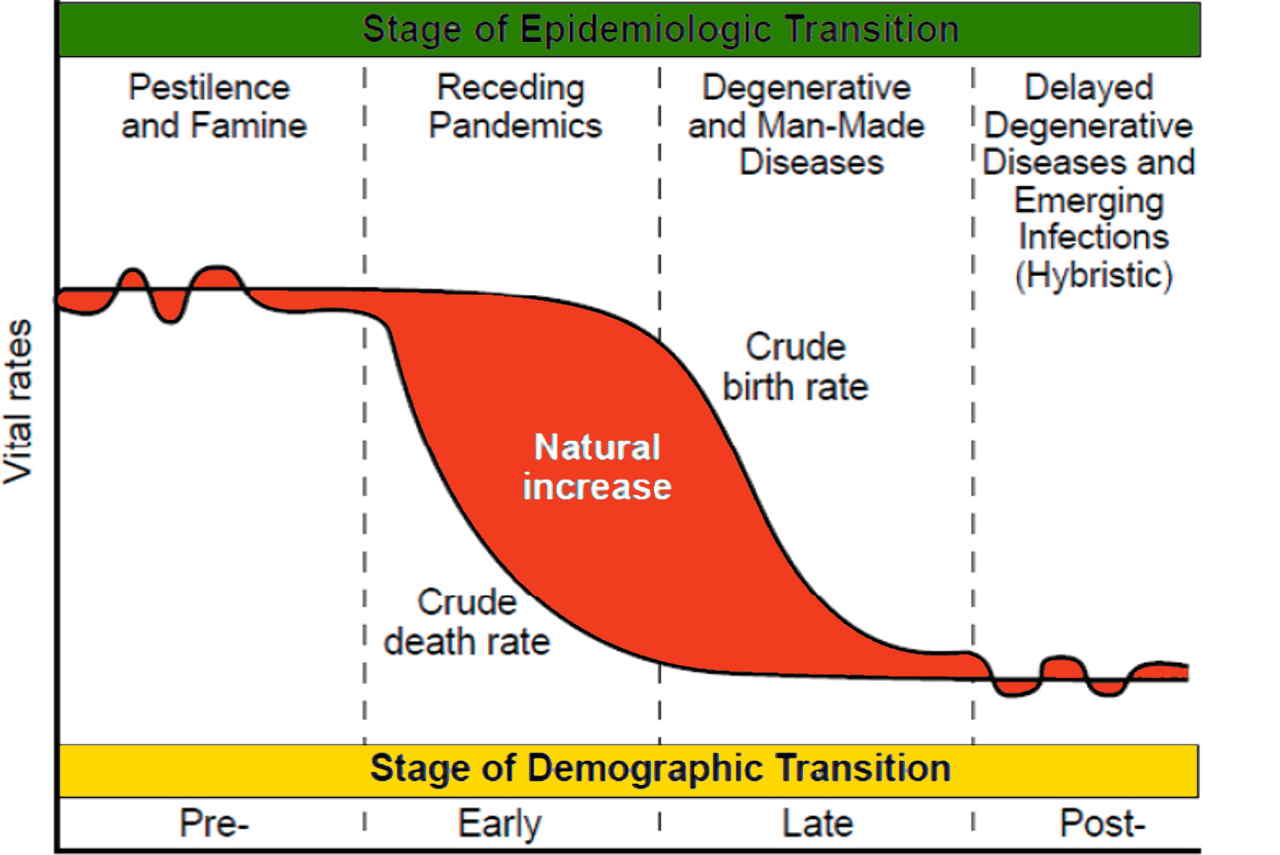
This study aims to examine epidemiologic transitions by identifying and quantifying the drivers of change in CVD risk in the middle-income country of South Africa compared to the high-income nation of England. It also aims to produce a harmonised dataset compiling national surveys measuring CVD risk factors in South Africa for others to use in future work.
Methods
We use microdata from nationally-representative surveys in South Africa and England. Data for South Africa derive from the Demographic and Health Surveys, National Income Dynamics Study, South Africa National Health and Nutrition Examination Survey and Study on Global Ageing and Adult Health, covering 11 cross-sections and approximately 180,000 individuals aged 15+ years, representing South Africa’s adult population from 1998 to 2017. Data for England come from 19 annual Health Surveys for England (HSE) over the same time, covering approximately 200,000 individuals aged 16+ years, representing England’s adult population. Area-level, local and environmental data from external sources supplement the analysis. The study uses multiple non-laboratory risk scores to estimate total CVD risk in the population and track its change over time. Trends in CVD risk and explanatory factors are first be explored in each country. Statistical modelling techniques, including fixed-effects, random-effects and structural equation modelling, will be used to examine to what extent various factors explain the variation in CVD risk over time.
Potential impact
The knowledge produced from this study can inform action at the governmental level (including health and social policy, services and planning) as well as at the societal level (including community awareness, provider practice and individual behaviour). As such, a range of stakeholders stand to benefit from this work, including policymakers and government bodies, civil society organisations, healthcare professionals, patient groups and the lay public. The evidence produced from our analysis can empower these stakeholders who are responsible for their personal as well as the public’s wellbeing. For instance, policymakers may use knowledge about the social, economic, demographic, behavioural, health and environmental drivers of CVD risk change to devise social policies addressing socioeconomic disadvantage, community deprivation, planning/development and health and social services to improve health. Doctors, nurses, community health workers and traditional practitioners may also benefit from this project through enhanced knowledge about the various factors influencing recent trends in CVD risk at the population level. This information can be used to advise patients and devise programmes and interventions to improve circulatory health. Therefore, there is potential for broad reach and significance of impact from this project.